Demonstrating the power and potential of dose-surface maps to investigate spatial effects of treatment planning parameters on delivered dose to the rectum
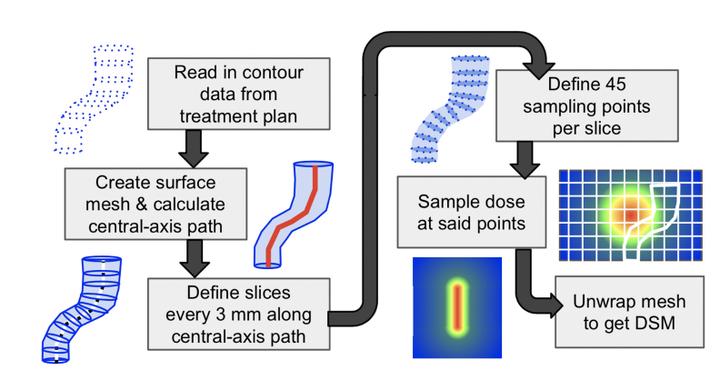 Image credit: Haley Patrick
Image credit: Haley PatrickAbstract
Purpose To demonstrate how dose-surface maps (DSMs) can be used to investigate the influence of PTV margins and fractionation schedules on the level of agreement between planned and delivered dose to the rectum during prostate radiotherapy. Methods Three retrospective prostate cancer cohorts treated with daily IGRT were used for this study:20 patients prescribed 36.25 Gy in 5 fractions with 5 mm PTV margins (5fx-5mm), 20 patients prescribed 60 Gy in 20 fractions with 7 mm margins (20fx-7mm), and the 20fx-7mm cohort replanned with 5 mm margins (20fx-5mm). The influence of margins was investigated using the 20fx-7mm and 20fx-5mm cohorts, and the influence of fractionation using the 5fx-5mm and 20fx-5mm cohorts. Delivered doses were determined by contouring daily CBCTs, registering planned beams to them, and calculating and summing rectum DSMs. Spatial agreement between planned and delivered DSMs was assessed using multiple-comparisons permutation testing. Results Both the 20fx-7mm and the 20fx-5mm cohorts were found to have significantly lower delivered doses than planned in similar subregions of the posterior rectum, indicating margin choice did not influence how planned and delivered doses differed. In contrast, the 5fx-5mm cohort had no significant differences between planned and delivered doses. While this suggests improved dose delivery with increased hypofractionation, an assessment of confounding factors is underway to draw firm conclusions. Conclusions DSM analysis revealed reduction of prostate PTV margins does not alter how planned and accumulated rectal wall doses vary spatially from each other. Further investigation is required to understand the influence of fractionation schedules.